Age-stratified analysis of patient and graft survival outcomes in donation after circulatory death versus donation after brain death kidney transplantation
Napat Leeaphorn1, Rose Mary Attieh1, Katherine M. Oshel1, Martin L. Mai1, Mary Prendergast1, Hani M. Wadei 1, Wisit Cheungpasitporn2, Tambi Jarmi 1.
1Transplant, Mayo Clinic Florida, Jacksonville , FL, United States; 2Division of Nephrology and Hypertension, Department of Medicine, Mayo Clinic Florida, Rochester , MN, United States
Background: While the impact of donation after circulatory death (DCD) kidneys on delayed graft function and death-censored graft failure (DCGF) is well-established, the mortality implications across different age groups, particularly in elderly recipients, remain understudied. We hypothesized that older recipients experience higher mortality when receiving DCD compared to donation after brain death (DBD) kidneys.
Methods: Using the UNOS/OPTN database, we analyzed deceased donor kidney transplants from 2015-2023 in recipients listed for kidney-only transplants with no prior solid organ transplantation history. Outcomes included patient survival (mortality) and death-censored graft failure, stratified by age ranges (20-30, 35-40, 45-50, 50-60, 60-70, 70-80 years). Inverse probability of treatment weighting (IPTW) was used to balance DCD and DBD groups within each age stratum, adjusting for recipient, donor, and immunosuppression characteristics. Cox proportional hazards models were used to estimate hazard ratios (HR) with 95% confidence intervals.
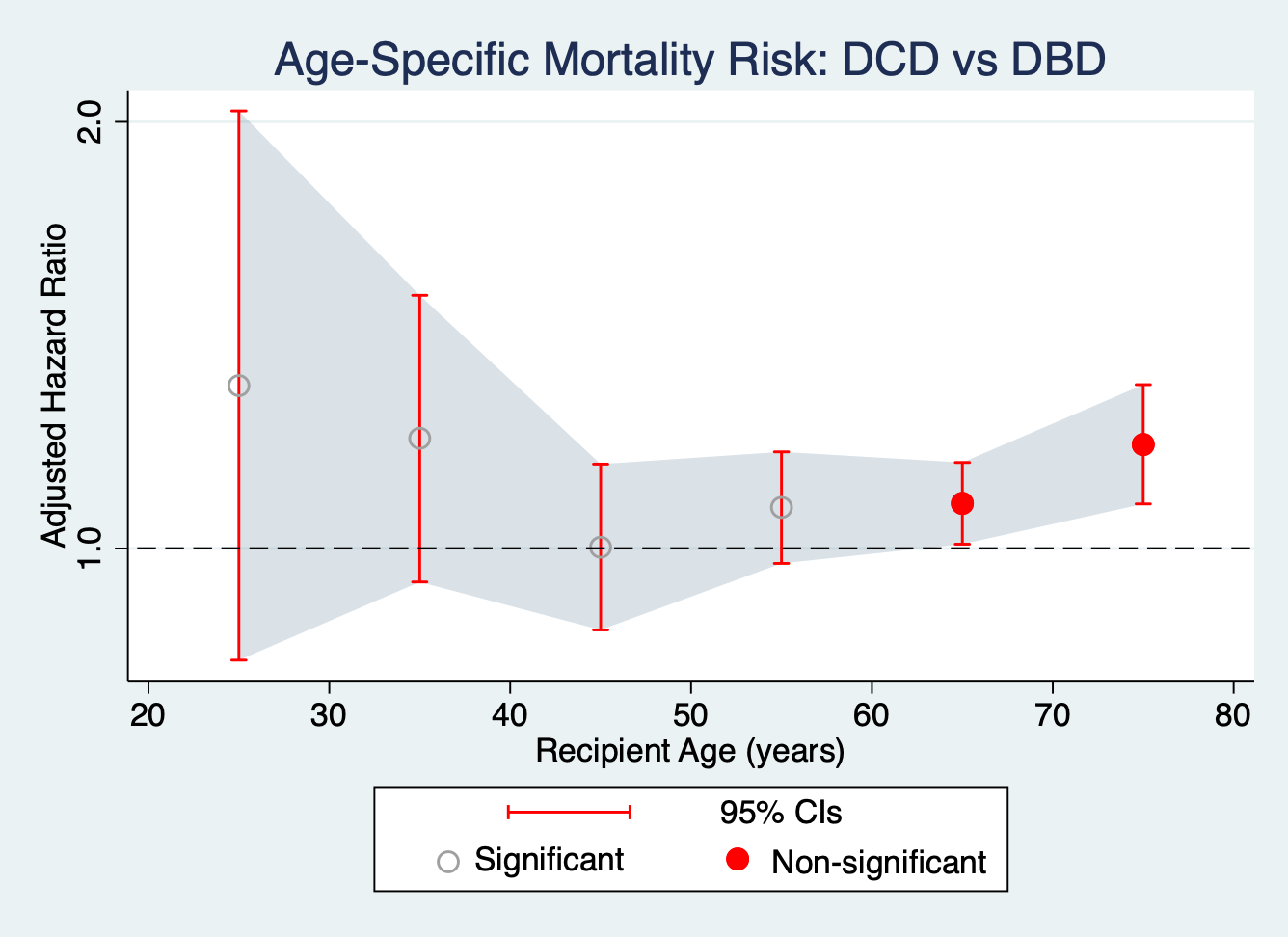
Results: A total of 116,396 kidney transplant recipients were analyzed across six age strata. For patient survival, DCD kidneys showed significantly increased mortality risk only in older recipients: ages 60-70 years (HR 1.08, 95% CI 1.01-1.15, p=0.03) and 70-80 years (HR 1.18, 95% CI 1.08-1.31, p=0.001). No significant mortality differences were observed in younger age groups (ages 20-60, all p>0.05). See Figure 1.
In contrast, death-censored graft failure showed a different pattern, with DCD kidneys demonstrating significantly higher graft failure risk across most age groups except for the youngest cohort (20-30 years). See Figure 2.
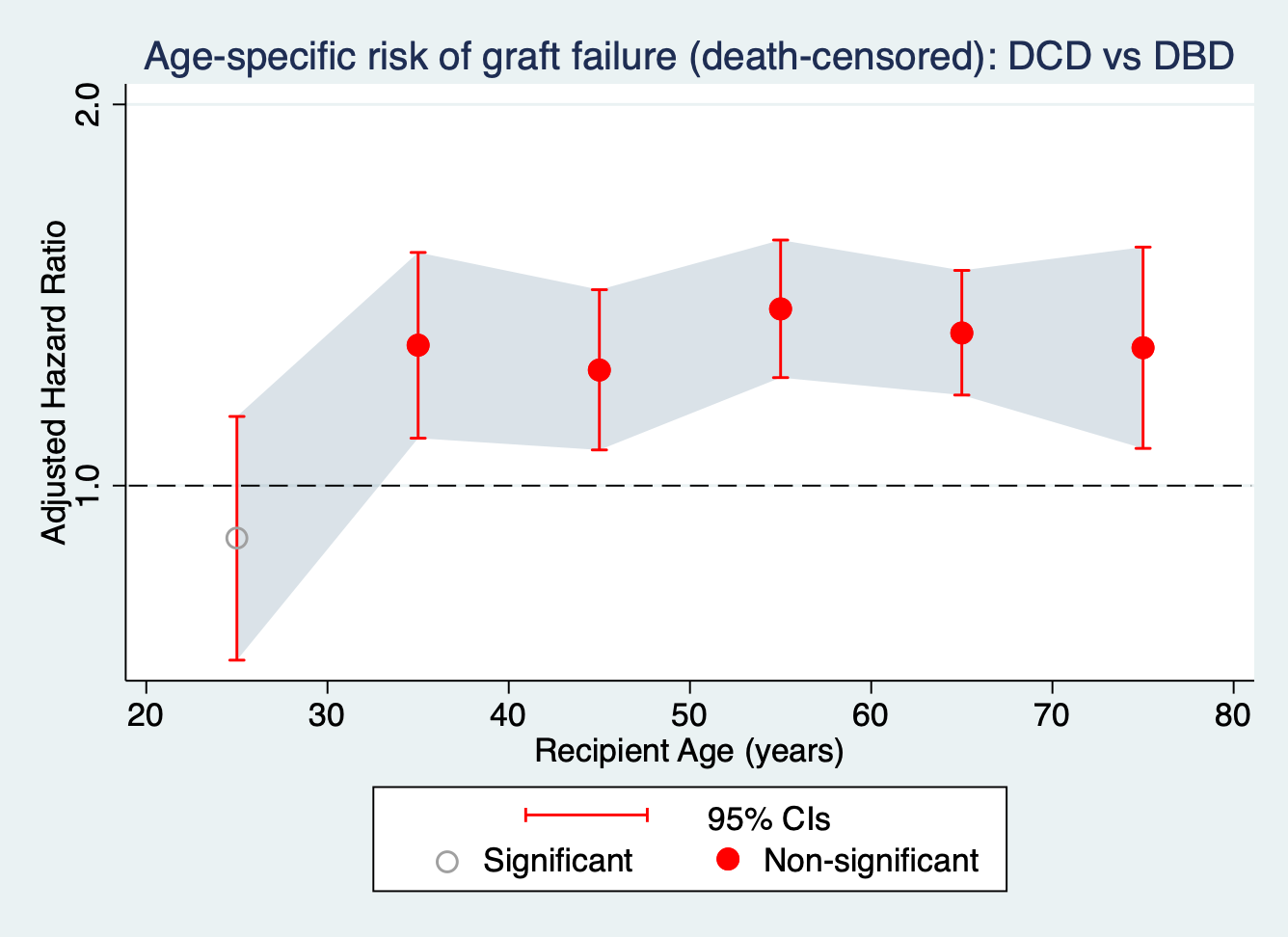
Conclusions: This large-scale analysis shows that the impact of DCD kidney transplantation varies by recipient age. DCD kidneys were associated with a higher risk of graft failure across most adult age groups, except the youngest recipients. Increased mortality risk was observed only in recipients aged 60 years and older, though the effect size was small despite statistical significance. Given the ongoing mortality risk of remaining on the waitlist, the benefits of accepting a DCD kidney may still outweigh the risks for most older candidates. These findings support the need for age-specific consideration and individualized risk–benefit discussions when evaluating DCD kidney offers. A separate target trial emulation is planned to compare outcomes of accepting a DCD kidney versus remaining on the waitlist in older kidney transplant candidates.
[1] OPTN
[2] DCD
[3] Kidney Transplantation
[4] Patient survival