Outcomes from a nascent A-NRP program—one OPO’s experience
Gennifer L Collins1, Michael P Lotts1, Rebecca J Roberts1, Gena M Mayer1, Tamer Malik1, Laia Coromina Hernandez1, David DeStefano1, Kenneth Woodside1.
1Sharing Hope South Carolina, Charleston, MI, United States
Introduction: Normothermic regional perfusion (NRP) is a rapidly expanding recovery practice that significantly impacts outcomes and utilization of organs procured from donation after circulatory death (DCD) organ donation cases. Herein, we describe our experience and outcomes for our nascent abdominal NRP (A-NRP) program.
Methods: Data on all A-NRP cases were collected following program initiation. Descriptive statistics were calculated for all data points collected.
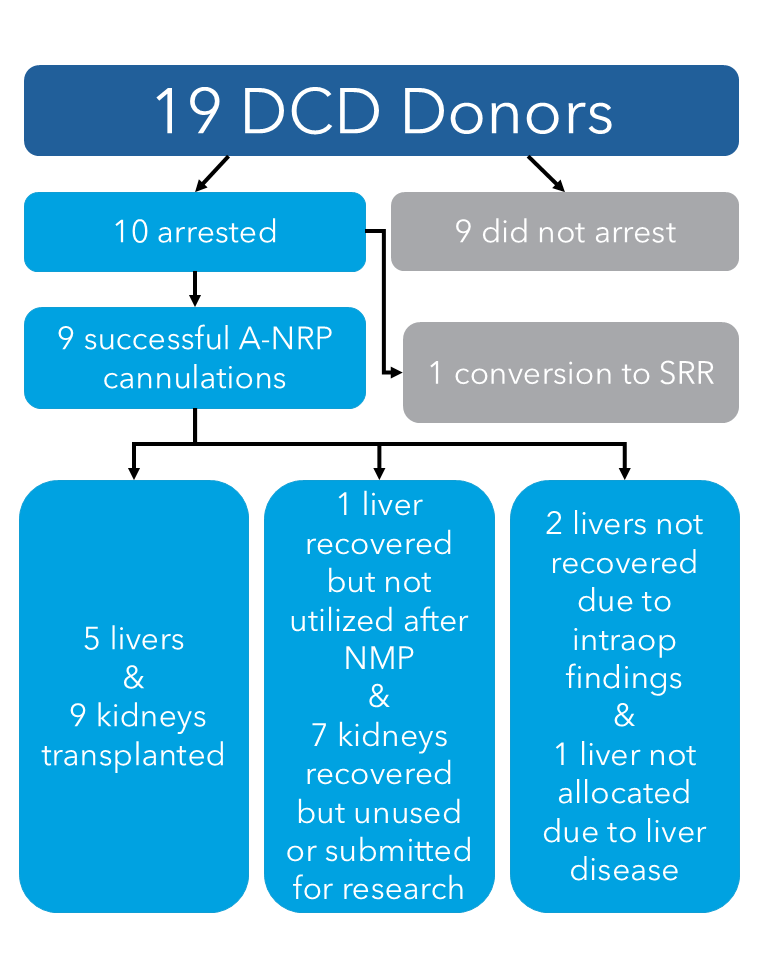
Results: The A-NRP program went live in November of 2024. Of the 19 cases attempted, 9 were completed, 9 did not arrest, and 1 case was started as A-NRP, but required transition to standard rapid recovery (SRR) at minute seven due to an air leak surrounding the pump’s venous cannula connection. Median age was 64 (range 48-75) and included 7 males and 12 females.
Of cannulated and pumped cases, the median age was 63 years (range 51-75), including 6 males and 3 females. Mean time from incision to cannulation was 5.88 min (range 5-9). Mean time on circuit was 95 min (range 63-144). A median of 4 PRBCs (range 0-6) were utilized. Lactate trends demonstrated either an overall reduction in value or appropriate increase associated with concurrent PRBC administration.
The 9 cases cannulated without transition to SRR resulted in transplant of 5 livers and 9 kidneys, with an additional liver recovered but unused after normothermic machine perfusion (NMP), another declined due to frank pus in the abdomen, and a third unrecovered after attempted salvage allocation (Figure). An additional 7 kidneys were recovered but not transplanted or went for research. Of note, 2 donors were over age 70 with one liver and two kidneys being transplanted.
Liver NMP was also used for 4 of the A-NRP cases following recovery. One case utilized A-NRP for abdominal organs but simultaneous SRR for thoracics. Use of concurrent NRP and NMP required extending OR times.
Conclusions: With careful planning, OPOs can successfully develop and implement A-NRP programs. Vigilant communication and collaboration are essential for programmatic success, particularly for cases with extended OR times. With support from hospital partners, we plan to expand the use of A-NRP for all adult DCD donors.
[1] Normothermic Regional Perfusion
[2] Normothermic Machine Perfusion
[3] Donation after Cardiac Death
[4] Organ Procurement Organization
[5] Abdominal Normothermic Regional Perfusion
[6] A-NRP
[7] NRP
[8] Liver
[9] Kidney
[10] Allocation