
Jeff is President and CEO of LifeShare Network and its subsidiary organizations, is President of the LifeShare Foundation, and consults nationally and internationally. Jeff has 38 years of experience in organ and tissue donation and a history of Board and community service. He currently serves as Vice President of the International Society for Donation Professionals, as a member of the MTF Biologics Board of Directors, as Vice Chair of the Donation Board of Trustees for MTF, and as Chair of the Oklahoma Governor’s Advancement of Wellness Advisory Council. He is a Past President of AOPO and of Donate Life America and has served multiple terms on the UNOS and OPTN Boards. He has been honored with numerous awards professionally and in the broader community. He has authored or coauthored numerous journal articles, has presented scientific abstracts and invited lectures around the world, and he is a Fellow of the American Society of Transplantation.
Rethinking normothermic liver perfusion: The case for organ procurement organizations as the ideal hub for ex vivo organ optimization
Clint A Hostetler1, Ashley N Milam1, Ronald A Squires1, Jeff P Orlowski1.
1Organ Recovery, LifeShare Network, inc., Oklahoma City, OK, United States
Background: The implementation of normothermic machine perfusion (NMP) for liver transplantation has largely been confined to transplant centers, following the precedent set by FDA clinical trials. This has reinforced the assumption that NMP must be performed within transplant programs, requiring the development of dedicated teams, a model that is often impractical for smaller centers due to resource limitations. To address this, a third-party nationalized service was introduced, providing organ recovery and perfusion. However, this model has been widely criticized for its excessive cost and limited long-term sustainability.
Methods: An alternative approach has been pioneered by an organ procurement organization (OPO) that became the first in the U.S. to independently own and operate an NMP device. By leveraging its existing infrastructure, including organ recovery surgeons, preservationists, and purpose-built facilities, the OPO successfully integrated NMP into its operations, demonstrating that perfusion could be effectively conducted outside transplant centers. This model enables costs to be distributed across all transplanted organs, significantly reducing the per-organ financial burden compared to a third-party service.
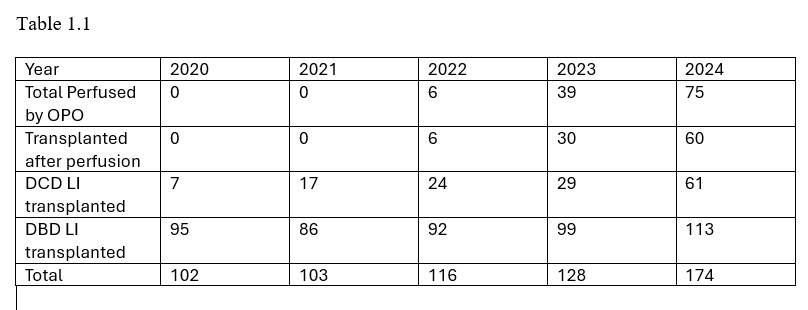
Results: Since implementing NMP with the OrganOx metra device in mid-2022, this OPO has achieved record-breaking increases in liver utilization, particularly for donation after circulatory death (DCD) grafts. Over two years, the number of NMP-perfused livers transplanted grew from 6 in 2022 to 60 in 2024 (Table 1.1), contributing to a substantial rise in overall liver transplant volumes. While liver organ acquisition costs (OAC) increased, spreading these costs across all organs resulted in a per-organ perfused and transplanted cost savings of approximately 50% compared to third-party NMP services. Additionally, the OPO partnered with the device manufacturer to establish a shared-risk model, ensuring that non-transplanted livers did not impose financial losses.
Conclusion: This OPO’s experience demonstrates that NMP can be successfully implemented within the OPO system, optimizing liver utilization while maintaining cost efficiency. By shifting NMP back to OPOs, where kidney perfusion has long been performed, this model promotes equitable access to cutting-edge organ preservation technologies, reduces financial strain on transplant centers, and ensures the sustainability of NMP. OPO-led NMP presents a scalable, cost-effective alternative that maximizes the gift of organ donation and advances the field of transplantation.
[1] Normothermic Machine Perfusion (NMP)
Liver Transplantation
Organ Procurement Organization (OPO)
Organ Preservation
Organ Recovery
Donation After Circulatory Death (DCD)
Donation After Brain Death (DBD)
Transplant Utilization
Cost Efficiency
Third-Party NMP Services
Shared-Risk Model
Organ Acquisition Costs (OAC)
Perfusion Technology
Sustainability in Transplantation
OPO-led NMP
Equitable Access to Transplantation
Liver Utilization Improvement
Healthcare Cost Reduction
Organ Preservation Innovations